The rectus diastasis
Content
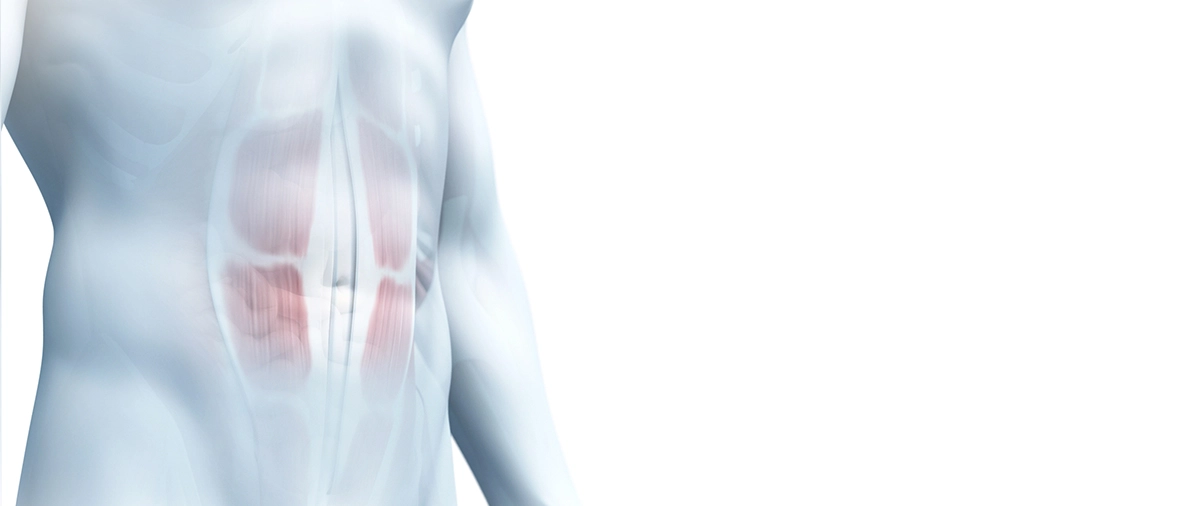
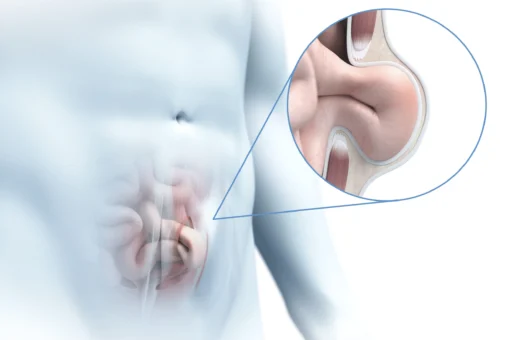
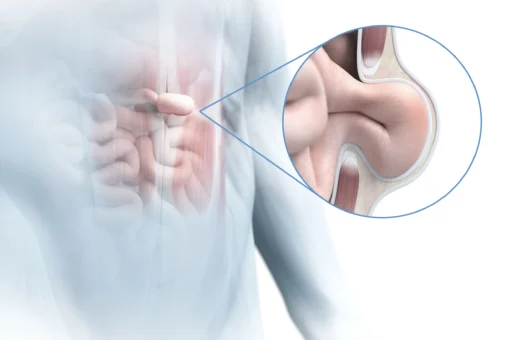
In rectus diastasis (midline hernia), the straight abdominal muscles separate increasingly. The intervening linea alba of connective tissue widens, becoming thinner and also more unstable. Normally 1 to 2 centimetres wide, the linea alba widens to up to 30 cm in a rectus diastasis.
Rectus diastasis is not a true hernia, but it increases the risk of abdominal wall hernias.
Rectus diastasis mainly occurs in women in the last third of pregnancy. The weight of the unborn baby causes the abdominal muscles to overstretch and separate. In addition, the hormone relaxin during pregnancy makes the abdominal muscles more elastic. Excess weight can also be a trigger for rectus diastasis.
Rectus diastases occur most often in the area of the navel. But they can also extend from the costal arch down to the pubic bone.
Rectus diastases are mostly acquired. Risk factors include obesity, heavy pushing during childbirth or chronic constipation and pregnancy. The age of the pregnant woman (over 35), a high weight of the newborn, multiple or multiple pregnancies and excessive abdominal muscle training in the first trimester can further increase the risk of rectus diastasis.
Symptoms of rectus diastasis
A rectus diastasis does not necessarily cause discomfort. However, the more pronounced it is, the more often the patient has to struggle with discomfort. Mostly, the rectus diastasis features also a visual-aesthetic problem. But when it is severe, support functions are also impaired. The muscle strength in the abdominal area, which is needed to stabilise the trunk, decreases as the front abdominal muscles move apart. This puts more strain on the back muscles. Patients with rectus diastases often complain of back pain because of this. The imbalance between the back and abdominal muscles also shows in the posture in a protrusion of the lumbar spine, which increases the well-known abdominal protrusion.
The doctor can feel the rectus diastasis. When the upper body is lifted, the intestines bulge forward. Sometimes the protrusion is also visible when standing.
- Protrusion on the anterior abdominal wall (bulbous abdomen, especially after eating)
- Palpable gap in the centre of the abdomen
- When stress is applied to the abdomen, the abdomen may bulge outwards or sink in
- Increased risk of abdominal wall hernias
- Pain during abdominal exercises
- Pain in the lower back, buttocks or hips (increased with physical exertion)
- Feeling of an unstable or soft body centre
- Weakening of the anterior abdominal wall stability
- Weak abdominal pressing
- Back pain
- Pelvic instability
- Pelvic floor weakness / difficulties with bowel movements
- Constipation, sometimes nausea
- Partial difficulties during birth, as the abdominal muscles are no longer strong enough to push the baby out
If an abdominal wall hernia forms due to the rectus diastasis and organ parts are trapped there, severe pain can occur. Incarcerated hernias must be operated on immediately. However, this occurs very rarely with rectus diastasis.
Classification of rectal diastases
Although rectus diastases are primarily perceived as cosmetically disturbing, from a certain degree of severity onwards they can be attributed a considerable disease value. Muscular trunk instability and consequently chronic back pain, as well as pelvic floor weakness, which can lead to incontinence, are the consequences of larger rectus diastases.
Rectus diastases are classified by the width of the linea alba, measured about 2 to 3 cm above the navel.
- W1 (smaller than 3 cm) – no to little skin overstretching – Regression recommended
- W2 (3 -5 cm) – little skin overstretching – Regression possible / surgery possible
- W3 (over 5 cm) – severe skin overstretching – Regression impossible / recommendation for surgery
In the case of a rectus diastasis W3, regression no longer makes sense because the straight abdominal muscles are already too far apart. In these cases, surgery is usually recommended and accordingly covered by the health insurance.
Treatment for rectus diastasis
Small rectus diastases that do not cause any discomfort do not need to be operated on. Rectus diastases can be treated by physiotherapeutic exercises of the abdominal muscles, as well as the trunk and pelvic muscles. However, this should only be done under the guidance of a specialist. If the wrong exercises are done, the rectus diastasis can even become larger and additional pressure is put on the pelvic floor.
The regression of a rectus diastasis after pregnancy takes time. The stretching of the linea alba recedes only slowly. 6 weeks after birth, 60% of women still have a rectus diastasis. One year after birth, 32% of women still have a rectus diastasis. For this reason, it makes sense to take preventive measures during pregnancy. In the last trimester, it is important to always roll onto your side first when getting up from lying down. Heavy lifting and sports that require a lot of strength should be avoided from the 5th month onwards.
We work closely with midwives, gynaecologists and physiotherapists and are in constant consultation with them to put together a targeted treatment program, individually for each patient. By means of physiotherapy, biofeedback training, strengthening of the trunk, pelvic and pelvic floor muscles, we can often avoid surgical intervention.
Surgery for rectus diastasis
In case of abdominal wall hernias, complications, trapped organ parts and severe discomfort, a rectus diastasis should be operated on. If the rectus diastasis is classified as W3, regression is no longer possible purely through physiotherapy and exercises. In this case, surgical treatment should be considered.
The surgeon uses internal sutures to fix the straight abdominal muscles back in their original position. Sometimes stabilising meshes are used.
Many patients who need to have a rectus diastasis surgically treated also have severe overstretching of the abdominal skin. If the patient wishes, an abdominoplasty can be performed at the same time. We will be happy to discuss the surgical options with you and advise you on your decision.
After the operation, the patient receives a supportive abdominal belt from us for about 2 weeks and then wears special compression underwear for about 6 weeks. It has been shown that these simple measures have a positive effect on the final result. After consultation, you can start exercising again as early as the 5th week.
You can find out more about the surgical procedures we practise here.

Contact us!
Read more about:
Spieghel's hernia is an abdominal wall hernia in which the hernial orifice is located approximately halfway between the navel and…
In the case of chronic groin pain, we use a detailed differential diagnosis to determine what is causing the pain.
Sportsman's groin, also known as "soft groin", often occurs in highly trained professional athletes and manifests itself in chronic, activity-related…

The diaphragm is a dome-shaped muscle and tendon tissue that separates the abdominal cavity from the chest cavity.

Parastomal hernias are hernias that occur next to an artificial bowel outlet (stoma).
Incisional hernias are hernias that occur in the area of a scar.
The navel is a natural weak point in the abdominal wall. A gap develops here when there is increased internal…
In femoral hernias, the peritoneum and sometimes loops of intestine push into the area of the thigh through a weak…
Inguinal hernias are divided into direct inguinal hernias, which are protruding through the abdominal wall towards the outside of the…