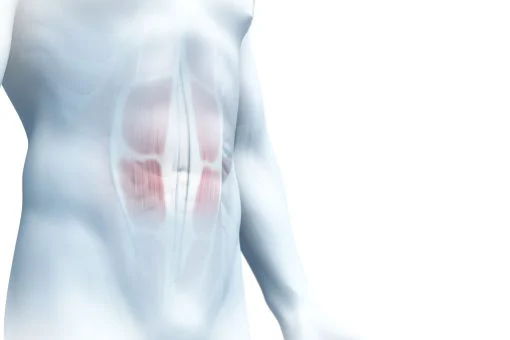
The incisional hernia
Content
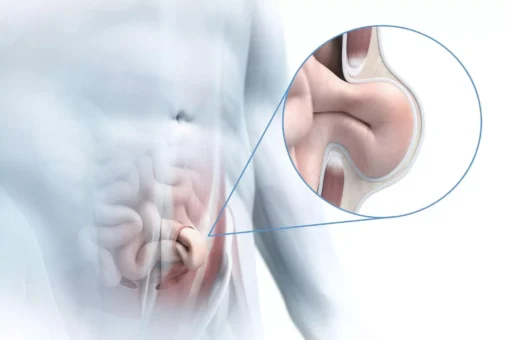
Incisional hernias are hernias that occur in the area of a scar. After abdominal wall surgery, there is a 10 to 20 per cent risk of scar hernias occurring later. Scar hernias are a common complication of abdominal wall surgery, but they only become noticeable in the longer term. Half of all scar hernias occur in the first six months after surgery. However, scar hernias can also develop up to five years after surgery.
Operations in which the abdominal wall layers have to be cut through in the middle of the abdomen along the body axis carry the greatest risk of later scar hernias. Decisive factors include the surgeon’s incision, the suture material used and the suturing technique.
Risk factors that favour the development of a scar hernia:
- Being overweight, as the pressure on the scar in the abdomen is increased
- Due to a larger proportion of fatty tissue, surgical wounds in overweight people can be sutured less precisely
- Repeated operations via the same surgical access
- Anaemia, as the scar tissue is supplied with too little oxygen and heals worse.
- Malnutrition
- Smoking (fourfold increased risk of scar fractures)
- Cortisone and other drugs that weaken the immune system
- Wound infections and wound healing disorders
- High age
- Hereditary collagen disorders
- Disorders of the connective tissue metabolism
- Peritonitis
- Diabetes
- Abdominal aortic aneurysm
The smaller the incisional hernia, the greater the risk of incarceration.
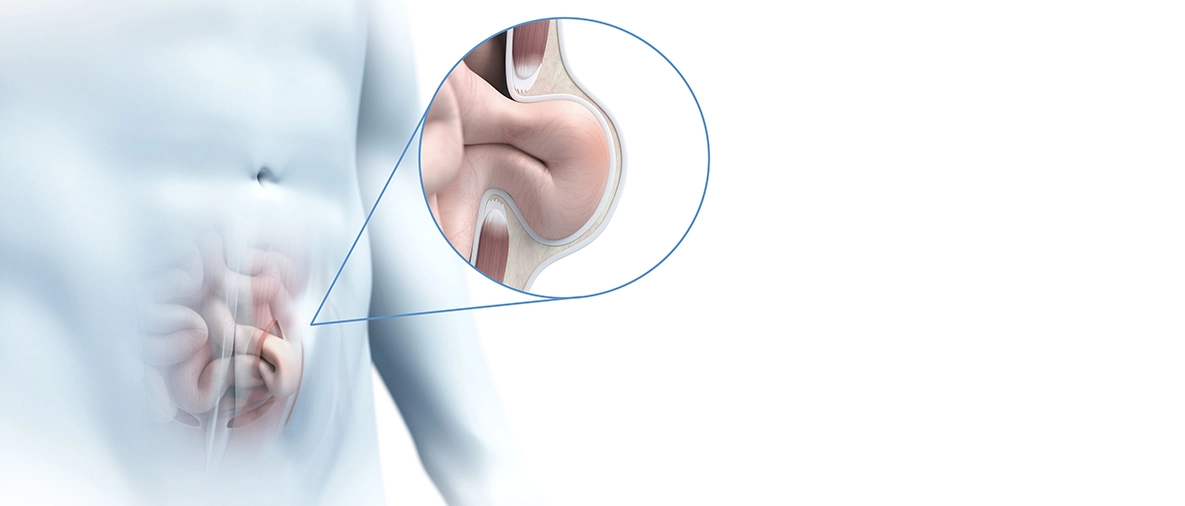
Symptoms of an incisional hernia
Depending on the size and location of the incisional hernia, there may be no symptoms at all or severe symptoms.
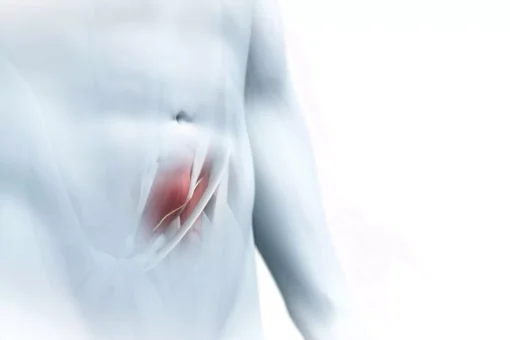
- Protrusion in the area of the scar
- Protrusion becomes more prominent with physical exertion
- Pain that occurs when lifting, pressing or coughing
- Pain during defecation
- Irregular bowel movements
- Blood in the stool
- Redness in the area of the hernia
- In the case of an incarceration, colicky abdominal pain, abdominal tenderness, fever and nausea.
CAUTION: If you have fever, vomiting, nausea and sudden colicky abdominal pain, it could be an incarcerated hernia. Call us immediately or go to the nearest hospital emergency ward!
To reduce the risk of an incisional hernia, it helps to lose weight and stop smoking if you are overweight before the operation. After abdominal wall surgery, stabilising abdominal bandages can be worn to relieve pressure on the tissue while the wound heals.
Surgery for an incisional hernia
Incisional hernias should always be operated on, as the scar tissue continuously drifts apart and the incisional hernia steadily enlarges.
Large incisional hernias often occur in severely overweight patients who have weak abdominal muscles and concomitant diseases. These are all risk factors for complications. In these cases, it makes sense to have the operation performed by specialists in a specialised hernia centre.
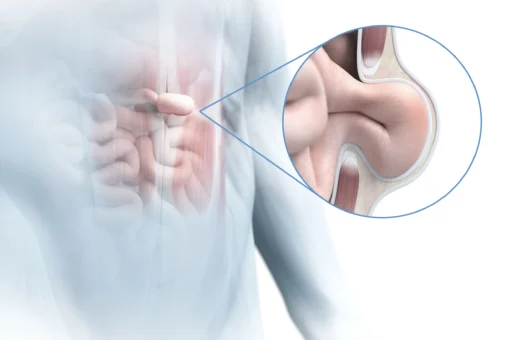
Scar hernias should be treated surgically at the earliest three to six months after the previous operation, otherwise the wound edges are not stable enough. Very small incisional hernias can be closed with a direct suture after the hernia sac has been pushed back into the abdominal cavity. For a gap of more than three centimetres, a mesh is usually inserted. It can be operated openly or minimally invasively.
Here you can find out more about the surgical techniques with or without mesh and the aftercare.

Contact us!
Read more about:
Spieghel's hernia is an abdominal wall hernia in which the hernial orifice is located approximately halfway between the navel and…
In the case of chronic groin pain, we use a detailed differential diagnosis to determine what is causing the pain.
Sportsman's groin, also known as "soft groin", often occurs in highly trained professional athletes and manifests itself in chronic, activity-related…
In rectus diastasis (midline hernia), the straight abdominal muscles separate increasingly.

The diaphragm is a dome-shaped muscle and tendon tissue that separates the abdominal cavity from the chest cavity.

Parastomal hernias are hernias that occur next to an artificial bowel outlet (stoma).
The navel is a natural weak point in the abdominal wall. A gap develops here when there is increased internal…
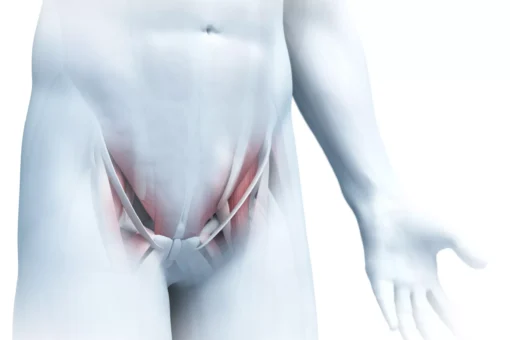
In femoral hernias, the peritoneum and sometimes loops of intestine push into the area of the thigh through a weak…
Inguinal hernias are divided into direct inguinal hernias, which are protruding through the abdominal wall towards the outside of the…